Clinical Scenario
ATLS & Polytrauma
Scenario
A 30-year-old male is involved in a road traffic accident, at approximately 60 mph, he is complaining of neck pain and pain in both hips. He has been air lifted to the nearest major trauma centre (MTC).
Interview Questions
How would assess this patient in the ED?
Key Concerns
-
High energy injury - ATLS Principles
-
Neck pain - requiring urgent C-spine stabilisation
-
Hip pain - suspicion of underlying pelvic ring injury
ATLS
“I would place a trauma call and ensure all members of the team had been assigned roles”
C-spine
-
Triple protection - collar / blocks / tape
Airway
-
Assess for stridor or upper airway sounds
-
Look for vomitus or blood in mouth - remove with yanker suction
-
If airway compromised proceed to airway management algorithm
-
Airway manoeuvres - jaw thrust (as patient C-spine immobilised)
-
Airway adjuncts (oro/nasopharyngeal airway)
-
Definitive airway - laryngeal mask airway or endotracheal tube
-
Surgical airway
-
-
Once happy with airway - 15L non-rebreathe mask + proceed
Breathing
-
Check oxygen (O2) saturations + respiratory rate (RR)
-
Focused respiratory examination
-
Inspect chest for signs of trauma - Ecchymosis / flail chest / open pneumothorax
-
Ensure trachea central
-
Equal chest expansion
-
Bilateral air entry
-
-
Order respiratory investigations (if indicated)
-
CXR
-
Arterial blood gas (ABG)
-
Circulation
-
Check heart rate (HR) and blood pressure (BP)
-
Focused cardiovascular examination
-
Check CRT - warm + well perfused? Cold clammy?
-
Heart Sounds
-
Assess for signs of haemorrhage
-
Chest
-
Abdomen
-
Pelvis
-
Long Bones
-
Surrounding patient
-
-
-
Gain intravenous (IV) access
-
Resuscitation fluids (20mls/Kg)
-
Order cardiovascular investigations
-
Trauma bloods: full blood count (FBC), urea and electrolytes (U+Es), liver function tests (LFTS), clotting, group and save (G&S)
-
ECG
-
VBG - lactate
-
Disability
-
Check:
-
Temperature - avoid hypothermia
-
Glasgow Coma Scale (GCS)
-
Glucose
-
Pupils
-
Exposure
-
Examine for other injury
-
Log roll patient - examine for spinal tenderness
-
If suspecting pelvic injury
-
Look for urethral injury - blood at urethral meatus / perineum bruising / high riding prostate
-
Perform rectal examination (PR) + vaginal examination (PV) - exclude open injury
-
The patient’s C-spine is stabilised. He has evidence of pelvic pain on examination and is currently hypotensive at 80/45 – what further blood loss management strategies would you consider?
If signs of haemodynamic compromise and a suspected pelvic fracture - prompt treatment is needed to prevent loss of life. Blood management strategies include:
-
IV resuscitation fluids
-
Blood product support
-
Activation of the major haemorrhage protocol
-
TXA - 1g IV stat (within 1 hour of injury) as per CRASH 2 Trial
-
Pelvic binder application
-
Focused Assessment with Sonography in Trauma (FAST) Scan - to identify if intra-abdominal / peritoneal bleeding
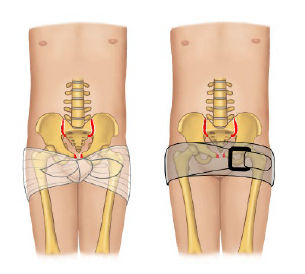
How would you apply a pelvic binder?
Pelvic binders help to compress the pelvic ring to prevent haemorrhage in patients with a suspected or confirmed pelvic fracture
Application:
-
Internally rotate the patient’s legs at the hips
-
Apply pelvic binder at the level of the greater trochanters
-
Tighten binder and secure into position
What is the major haemorrhage protocol?
The major haemorrhage protocol is an emergency blood order for patients with major haemorrhage / uncontrollable bleeding. It alerts and mobilises individuals needed to deliver blood products rapidly.
Including:
-
Porters
-
Blood transfusion lab technicians
-
On-call haematologist
Consists of two packs containing the necessary blood products (the constituents of these packs vary – based on local hospital policy)
Example
-
Pack A (4:4:1 ratio)
-
Packed Red Cells : Fresh Frozen Plasma : Platelets
-
-
Pack B (4:4:2:1 ratio)
-
Packed Red Cells : Fresh Frozen Plasma : Cryoprecipitate : Platelets
-
The patient has received 2 units of blood within 30 minutes of arriving in the department. Name 3 potential transfusion problems?
-
Pyrexia
-
Immediate Haemolytic transfusion reaction: Due to ABO incompatibility
-
Hypocalcaemia: Due to chelating agent
-
Hyperkalaemia: Released from RBCs stored too long
-
TACO (Transfusion associated circulatory overload): Due to too much blood transfused
-
TRALI (Transfusion associated lung injury (ARDS like picture): Non-cardiogenic cause of pulmonary oedema
-
Hypothermia: From unwarmed blood transfused after keeping blood in fridge
-
Anaphylaxis
-
Infective / bacterial shock: Hep B / Hep C / HIV / Syphillis / vCJD
-
CMV (more common than others à can be disastrous in immunocompromised)
-
-
Graft Vs host disease: Due to HLA mis-match
Note: This is why we give warmed bloods to prevent hypothermia, also need to monitor electrolytes (Ca and K+) following massive transfusions
What are the different classifications of haemorrhagic shock?
Look at images section -> haemorrhagic shock table
Remember that blood pressure only starts to reduce at STAGE 3 shock
What signs would be present in hypovolaemic shock?
SHOCKS
S Sinus tachycardia
H Hypotension
O Oliguria
CK Cold and Klammy peripheries
S Slow cap refill
What other injuries do you need to evaluate for in pelvic trauma?
-
Vascular Injury
-
Thorough haemorrhage assessment should be performed as part of ATLS
-
Blood loss management strategies should be activated
-
Escalation to consultant early
-
-
Urological injury
-
Signs include - blood at urethral meatus / perineum bruising / high riding prostate
-
Should be managed as per BOAST: The Management of Urological Trauma Associated with Pelvic Fractures [1]
-
Ensure discussed with on-call urology SpR
-
-
Open Injuries
-
Need to exclude open rectal or vaginal injury
-
Ensure PR and PV performed in ED
-
If blood present on examination - treat as open fracture. Manage as per BOAST: Open Fractures [2]
-
What is the lethal triad in trauma?
The lethal triad in trauma consists of:
-
Hypothermia
-
Coagulopathy
-
Acidosis
It is seen in patients with severe polytrauma and results in a significant rise in mortality rate when present. Works as a positive feedback loop where one factors causes a deterioration of another and so on
What is the role of tranexamic acid (TXA) in trauma? What time frame should it be given in?
-
TXA works by antifibrinolytic activity by reversibly binding to plasminogen
-
This prevents formation of plasmin therefore preventing fibrin clot degradation
-
-
All trauma patients with blunt or penetrating trauma should receive TXA
-
1g IV given over 10 minutes
-
Increasingly given pre-hospital by paramedics
What were the findings of the CRASH-2 Trial?
The CRASH-2 (Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage) trial [3] was a large, international, randomised controlled trial conducted to evaluate the efficacy and safety of tranexamic acid (TXA) in patients with trauma.
Summary
-
The CRASH-2 trial assessed TXA in trauma patients.
-
Over 20,000 participants from various countries were involved.
-
TXA administered within 3 hours of injury reduced bleeding-related mortality by about one-third.
-
There was no increase in adverse events such as thromboembolic events.
-
These findings have led to the widespread adoption of early TXA administration in trauma care protocols worldwide.
What is the difference between early total care (ETC), damage control orthopaedics (DCO) and early appropriate care?
Early Total Care (1970s)
-
ETC was introduced in 1970s
-
Aim was rapid stabilisation of all long bone fractures within 24 hours once patient was physiologically safe
-
This went out of fashion due to concerns regarding “Second Hit Hypothesis”
Damage Control Orthopaedics (1990s)
-
DCO is a concept introduced in 1990s to replace early total care
-
With the aim of avoiding the second hit hypothesis by performing only limb or life-threatening surgery
-
Definitive fixation is the delayed until patient is physiologically stable - therefore attempting to give the patient physiological reserve to cope with major surgery
Early Appropriate Care (2010s)
-
Hybrid of ETC and DCO concepts
-
Aim to perform as much surgery as possible once patient physiologically safe
-
Some MTCs now using lactate as a marker of physiological stability - using it to determine whether a patient is suitable for ETC or DCO
-
Lactate <2mmol/L - appropriate for ETC
-
Lactate >2.5mmol/L - resuscitation +/- conversion to DCO approach
-
-
Monitoring of lactate may be done in theatre with aggressive resuscitation and stopping of surgery if patients lactate rising too high
What are the aims of damage control orthopaedics?
-
Time limited interventions (not definitive)
-
Minimise second physiological hit
-
Aiming to perform life and limb saving procedures
-
Stabilising the patient until definitive fixation can take place
Give some examples of damage control orthopaedic interventions
-
Haemorrhage control (packing / CT embolization / pelvic external fixation)
-
Debridement of open fractures
-
Decompressive fasciotomies
-
Reduction of dislocated joints
-
Stabilising fractures (traction / external fixation / POP)
What is the “second hit hypothesis”?
Second Hit Hypothesis
-
Second hit hypothesis is that major trauma results in an initial physiological insult (or hit)
-
Major surgery rapidly following this can result in a SECOND physiological insult to the patient
-
Causing reactivation of the systemic inflammatory response and lead to syndromes such as adult respiratory distress syndrome or multi-organ dysfunction syndrome.
References
[1] BOA. BOAST – The Management of Urological Trauma Associated with Pelvic Fractures. Available at: https://www.boa.ac.uk/resources/boast-14-pdf.html
[2] BOA. BOAST – Open Fractures. Available at: https://www.boa.ac.uk/resources/boast-4-pdf.html
[3] Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17(10):1-79.
Images